
No products in cart

Could a Hidden Infection Be Affecting Fertility and Reproductive Health?
Oophoritis is an inflammation of the ovaries caused by an infection. The condition may affect one ovary or both. It often occurs together with inflammation of the fallopian tubes (salpingitis); in such cases, the condition is called salpingo-oophoritis or adnexitis. Ovarian inflammation can pose a serious risk to a woman’s reproductive health and fertility.
Causes
The inflammatory process may be:
- Specific, caused by pathogenic microorganisms such as chlamydia, Mycobacterium tuberculosis (Koch’s bacillus), Trichomonas, mycoplasmas, or gonococcal infection.
- Nonspecific, resulting from the overgrowth of opportunistic microorganisms such as Candida species or Escherichia coli.
Factors that can contribute to inflammation of the ovaries and fallopian tubes include hypothermia, gynecological diagnostic or surgical procedures, use of an intrauterine device (IUD), childbirth, abortion procedures, and menstruation. Infection often spreads upward from the cervix, uterus, or fallopian tubes. In some cases, pathogens reach the adnexa through the bloodstream or lymphatic system, which is typical of tuberculosis.
Symptoms
Oophoritis may occur in acute, subacute, or chronic forms, each with distinct characteristics.
Acute oophoritis is typically characterized by severe, persistent pain in the lower abdomen on one or both sides, often radiating to the lower back or sacral area. Other symptoms may include frequent and painful urination, abnormal serous or purulent vaginal discharge, fever, chills, general malaise, pain during sexual intercourse, and spotting between menstrual periods. During a gynecological examination, enlarged and tender ovaries are usually detected. Acute ovarian inflammation generally requires hospital treatment, and prompt therapy greatly increases the likelihood of complete recovery.
If inadequately treated, the disease may become chronic, with periods of relapse. Chronic oophoritis often causes dull, aching pain in the lower abdomen, groin, or vaginal area that may worsen before menstruation or after exposure to cold. Women may also experience menstrual irregularities, vaginal discharge, decreased libido, painful intercourse, and difficulty conceiving despite regular sexual activity. Chronic inflammation can affect emotional well-being, leading to irritability, sleep disturbances, fatigue, and reduced work capacity.
In some cases, especially with certain sexually transmitted infections, chronic inflammation may be asymptomatic. Without treatment, there is an increased risk of fallopian tube obstruction and pelvic adhesions, both of which can contribute to infertility.
Subacute oophoritis is relatively uncommon and is most often associated with fungal or tuberculous infections.
Diagnosis
Diagnosing oophoritis can be challenging because its symptoms may resemble those of other conditions that cause acute abdominal pain, such as appendicitis, endometriosis, ovarian cyst inflammation, ectopic pregnancy, or peritonitis.
Diagnosis typically begins with a detailed gynecological and medical history, including previous illnesses, procedures, and current symptoms. Laboratory tests often reveal elevated white blood cell counts in blood, urine, or vaginal smear samples. A bimanual pelvic examination may show enlarged, tender ovaries and fallopian tubes.
Additional diagnostic methods may include PCR testing, ELISA, and bacteriological studies to identify specific infectious agents. Ultrasound can help confirm ovarian inflammation, while hysterosalpingoscopy may detect structural abnormalities of the fallopian tubes. Laparoscopy is considered one of the most informative diagnostic procedures, especially in chronic cases, as it can reveal adhesions, pus accumulation, and tubal blockage.
Treatment
Treatment should begin only after a definitive diagnosis has been established. The approach depends on the stage of the disease, symptoms, and the underlying cause.
Women with acute oophoritis are usually hospitalized and prescribed bed rest. Treatment commonly includes antibiotics or other antimicrobial medications to eliminate the infection, anti-inflammatory therapy, pain relief, and supportive medications such as desensitizing agents, sulfonamides, and immune-supportive therapies. During the first few days, cold compresses may be applied to the lower abdomen to reduce inflammation.
Once the infectious agent has been identified, antibiotic therapy is tailored according to the organism’s sensitivity profile. In chronic cases, treatment aims to eliminate infection, reduce inflammation, relieve symptoms, strengthen immunity, and restore ovarian function.
After acute inflammation subsides, physiotherapy may be recommended. Common methods include laser therapy, electrophoresis, and magnetic therapy. To reduce the risk of adhesions and tubal obstruction, some patients may undergo gynecological massage, therapeutic mud treatments, or hirudotherapy (leech therapy). Acupuncture may also be used to help manage chronic pelvic pain. In recurrent cases, immunomodulatory medications may be prescribed to enhance immune function.
Advanced or neglected cases can be more difficult to treat and may require surgical intervention if complications develop.
Prevention
To reduce the risk of ovarian and fallopian tube inflammation, women are advised to:
- Avoid hypothermia.
- Maintain good personal hygiene.
- Minimize stress whenever possible.
- Avoid excessive physical and emotional exhaustion.
- Have regular gynecological checkups, ideally every six months.
- Avoid casual or unprotected sexual encounters.
- Follow a balanced and nutritious diet.
- Use effective contraception to prevent unintended pregnancy and reduce the risk of sexually transmitted infections.
Many symptoms of oophoritis—such as pelvic pain, irregular periods, fatigue, or discomfort during sex—can be mistaken for other conditions. Why do you think reproductive health issues are often overlooked or diagnosed late, and what steps can women take to recognize warning signs and seek timely medical care?


Lia
Founder & Editor Lia is a biologist with many years of research experience and a deep love for natural medicine. She is passionate about natural remedies, healthy living, and simple ways to support the body through nature. Eager to share her knowledge, Lia enjoys offering helpful lifestyle tips, wellness tricks, natural recipes passed down through generations, and inspiring ideas for living a healthier and more balanced life.Related Posts

Anovulatory Cycles and Infertility: What Every Woman Should Know
June 24, 2026
Anovulatory cycles happen when the ovaries do not release an egg, which can make it harder to predict periods and conceive naturally. Although some cycles may look normal, irregular ovulation...
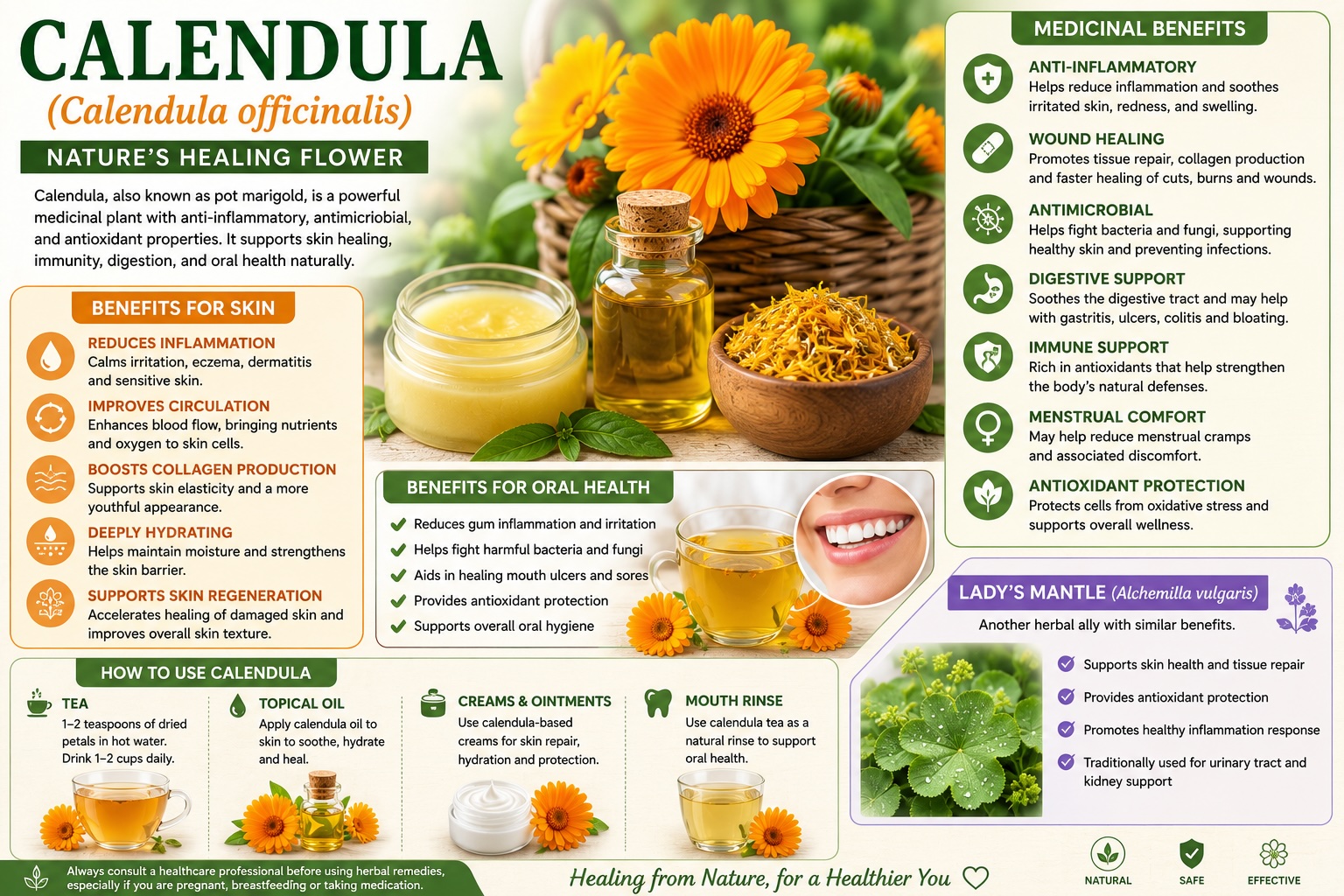
Calendula Benefits for Skin, Immunity, and Oral Health: A Complete Guide
June 23, 2026
Calendula is a bright, healing flower known for its soothing, antioxidant-rich properties. From calming irritated skin to supporting the body’s natural immune defenses and promoting oral comfort, calendula has been...

Simple Ways to Ease Gum Pain Naturally
June 23, 2026
Experiencing sore or swollen gums? Learn the most common causes of gum pain, simple home remedies that can provide relief, and the warning signs that mean it's time to see...
Leave a Comment